
























Nori Human Hemopexin ELISA Kit

Price range: $508.00 through $916.00
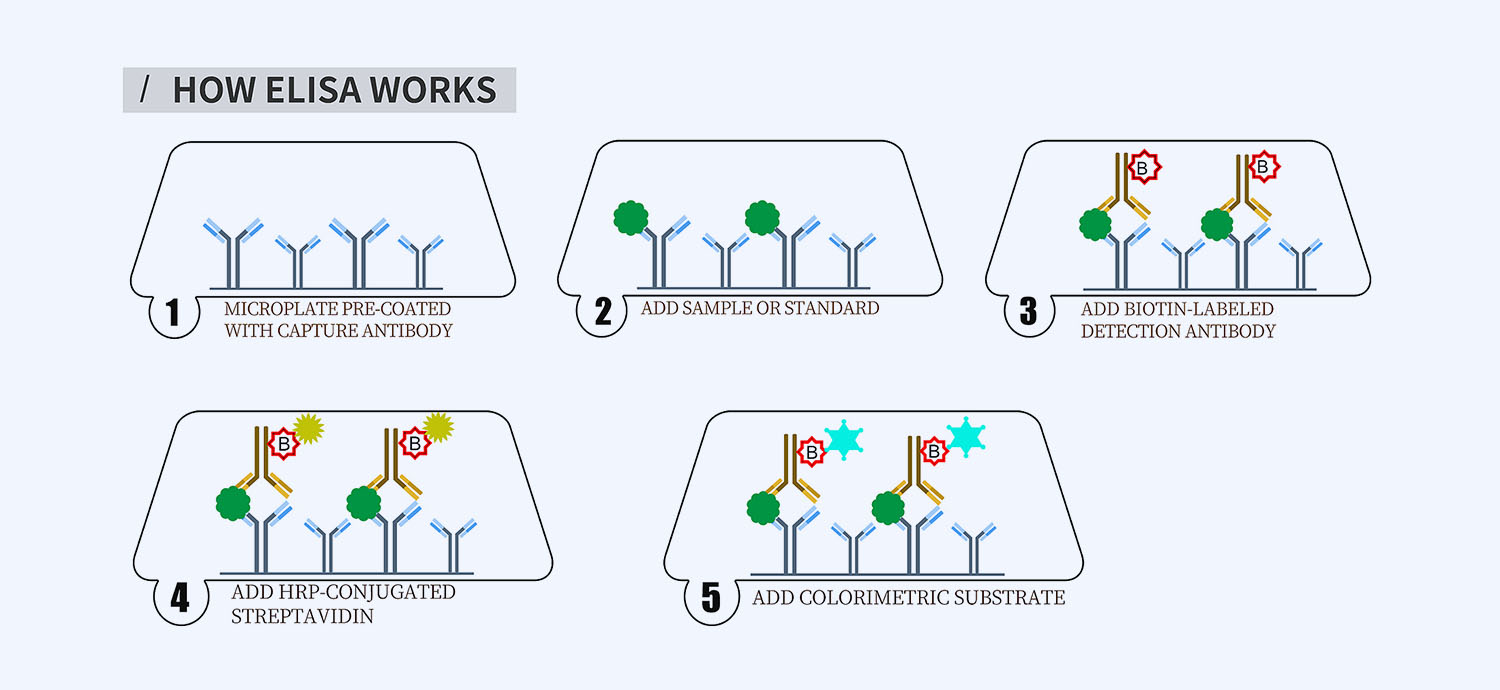
This ELISA kit is for quantification of hemopexin in human. This is a quick ELISA assay that reduces time to 50% compared to the conventional method, and the entire assay only takes 3 hours. This assay employs the quantitative sandwich enzyme immunoassay technique and uses biotin-streptavidin chemistry to improve the performance of the assays. An antibody specific for HPX has been pre-coated onto a microplate. Standards and samples are pipetted into the wells and any HPX present is bound by the immobilized antibody. After washing away any unbound substances, a detection antibody specific for HPX is added to the wells. Following wash to remove any unbound antibody reagent, a detection reagent is added. After intensive wash a substrate solution is added to the wells and color develops in proportion to the amount of HPX bound in the initial step. The color development is stopped, and the intensity of the color is measured.
Alternative names for hemopexin: HPX, HX, haemopexin, beta-1B-glycoprotein
This product is for laboratory research use only not for diagnostic and therapeutic purposes or any other purposes.
- Description
- How Elisa Works
- Documents
- Product Citations
- Reviews (0)
Description
Nori Human Hemopexin ELISA Kit Summary
Alternative names for hemopexin: HPX, HX, haemopexin, beta-1B-glycoprotein
| Assay Type | Solid Phase Sandwich ELISA |
| Format | 96-well Microplate or 96-Well Strip Microplate |
| Method of Detection | Colorimetric |
| Number of Targets Detected | 1 |
| Target Antigen Accession Number | P02790 |
| Assay Length | 3 hours |
| Quantitative/Semiquantitative | Quantitative |
| Sample Type | Plasma, Serum, Cell Culture, Urine, Cell/Tissue Lysates, Synovial Fluid, BAL, |
| Recommended Sample Dilution (Plasma/Serum) | No dilution for sample <ULOQ; sufficient dilution for samples >ULOQ |
| Sensitivity | 150 pg/mL |
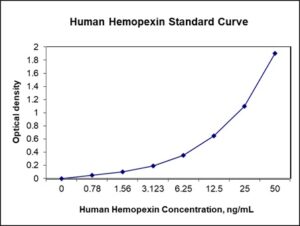
| Detection Range | 0.78-50 ng/mL |
| Specificity | Human HPX |
| Cross-Reactivity | < 0.5% cross-reactivity observed with available related molecules, < 50% cross-species reactivity observed with species tested. |
| Interference | No significant interference observed with available related molecules |
| Storage/Stability | 4 ºC for up to 6 months |
| Usage | For Laboratory Research Use Only. Not for diagnostic or therapeutic use. |
| Additional Notes | The kit allows for use in multiple experiments. |
Standard Curve
Kit Components
1. Pre-coated 96-well Microplate
2. Biotinylated Detection Antibody
3. Streptavidin-HRP Conjugate
4. Lyophilized Standards
5. TMB One-Step Substrate
6. Stop Solution
7. 20 x PBS
8. Assay Buffer
Other Materials Required but not Provided:
1. Microplate Reader capable of measuring absorption at 450 nm
2. Log-log graph paper or computer and software for ELISA data analysis
3. Precision pipettes (1-1000 µl)
4. Multi-channel pipettes (300 µl)
5. Distilled or deionized water
Protocol Outline
1. Prepare all reagents, samples and standards as instructed in the datasheet.
2. Add 100 µl of Standard or samples to each well and incubate 1 h at RT.
3. Add 100 µl of Working Detection Antibody to each well and incubate 1 h at RT.
4. Add 100 µl of Working Streptavidin-HRP to each well and incubate 20 min at RT.
5. Add 100 µl of Substrate to each well and incubate 5-30 min at RT.
6. Add 50 µl of Stop Solution to each well and read at 450 nm immediately.
Background:
Hemopexin (haemopexin; Hpx; Hx), also known as beta-1B-glycoprotein, is a glycoprotein that is encoded by the HPX gene[1] and belongs to the hemopexin family of proteins. Hemopexin is a plasma protein with the highest binding affinity for heme and is the major vehicle for the transportation of heme in the plasma.[2] Human plasma Hx consists of a single polypeptide chain of 439 amino acids residues with six intrachain disulfide bridges and has a molecular mass of approximately 63 kD. Its main function is scavenging the heme released or lost by the turnover of heme proteins such as hemoglobin and thus protects the body from the oxidative damage that free heme can cause. In addition, Hx releases its bound ligand for internalisation upon interacting with CD91.[3] Hx preserves the body’s iron.[2] Hx-dependent uptake of extracellular heme can lead to the deactivation of Bach1 repression which leads to the transcriptional activation of antioxidant heme oxygenase-1 gene. Hemoglobin, haptoglobin (Hp) and Hx associate with HDL and influence the inflammatory properties of HDL.[4] Hx can downregulate the angiotensin II Type 1 receptor (AT1-R) in vitro.[5] The predominant source of circulating Hx is the liver with a plasma concentration of 1–2 mg/ml.[6] Serum Hx level reflects how much heme is present in the blood. Therefore, a low Hx level indicates that there has been significant degradation of heme containing compounds. A low Hx level is one of the diagnostic features of an intravascular hemolytic anemia. Hx has been implicated in cardiovascular disease, septic shock, cerebral ischemic injury, and experimental autoimmune encephalomyelitis.[7] The circulating level of Hx is associated with prognosis in patients with septic shock.[7] HPX is produced in the brain.[8] Deletion of the HPX gene can aggravate brain injury followed by stroma-free hemoglobin-induced intracerebral haemorrhage.[9] High Hx level in the cerebrospinal fluid is associated with poor outcome after subarachnoid hemorrhage.[8] *Both Hp and Hx are acute-phase proteins, the synthesis of which are induced during infection and after inflammatory states to minimize tissue injury and facilitate tissue repair.[2] Hp and Hx prevent heme toxicity by binding themselves to heme prior to monocyte or macrophage‘s arrivals and ensuing clearances.[2]
References
- Altruda F, et al. (1985). Nucleic Acids Research. 13 (11): 3841–59.
- Tolosano E, Altruda F (April 2002). “Hemopexin: structure, function, and regulation”. DNA and Cell Biology. 21 (4): 297–306.
- Hvidberg V, et al. (2005). Blood. 106 (7): 2572–9.
- Watanabe J, et al. (2009). The Journal of Biological Chemistry. 284 (27): 18292–301.
- Krikken JA, et al. (2013). Journal of Hypertension. 31 (3): 537–41.
- Muller-Eberhard U, et al. (1968). Blood. 32 (5): 811–5.
- Mehta NU, Reddy ST (2015). Current Opinion in Lipidology. 26 (5): 384–7.
- Garland P, et al. (2016). Stroke. 47 (3): 872–6.
- ^Ma B, et al. (2016). Journal of Neuroinflammation. 13: 26.
Product Citations
Be the first to review “Nori Human Hemopexin ELISA Kit”
You must be logged in to post a review.
Reviews
There are no reviews yet.